A Longitudinal Study of the Effect of Renal Failure on Readmission Rates of Patients with Clostridium Difficile
Brian Detweiler
May 4, 2018
Hello and thank you for coming!
Alternative titles
- How to lose friends and infect people
- Epidemiology! For fun and for profit





About me
- University of Nebraska, Omaha
- B.S. Computer Science and Mathematics (2009)
- M.S. Mathematics, Data Science (May, 2018)
- Software Engineer (2004-present)
- Flight Operations, U.S. Army National Guard (2000-2009)



Agenda
- Introduction and motivation
- C. diff and renal failure
- The data
- Methodology
- Results
Introduction and motivation
Why are we here?
Pr(You)
- \(Pr(\text{boy meets girl}) = \frac{1}{20000}\)
- \(Pr(\text{same boy knocks up same girl}) = \frac{1}{2000}\)
- \(Pr(\text{right sperm meets right egg})\) = 1 in 400 quadrillion
- \(Pr(\text{lineage})\): 1 in \(10^{45000}\)
- \(Pr(\text{you})\) = 1 in \(10^{2685000}\)
So what’s the probability of your existing? It’s the probability of 2 million people getting together – about the population of San Diego – each to play a game of dice with trillion-sided dice. They each roll the dice, and they all come up the exact same number – say, 550,343,279,001.
A miracle is an event so unlikely as to be almost impossible. By that definition, I’ve just shown that you are a miracle.
Benazir, A. What are the chances of your coming into being? (2011)
Data Science
Big Data
- Volume
- How big is BIG? Gigabytes? Petabytes? Exabytes?
- Velocity
- Twitter averages 5,700 tweets/second
Kirkorian, R. New Tweets per second record, and how! (2013)
- Twitter averages 5,700 tweets/second
- Variety
- Plain text, XML, JSON, video, audio, etc.
- And sometimes veracity
- Questionable data quality
Finding a project
- 🚫 Union Pacific PTC data (2016-2017) - SCRAPPED
- ✅ HCUP project through Creighton
C. diff and renal failure
C. diff
- Clostridium difficile
- Gram-positive, anaerobic, rod-shaped, Endospore-forming bacterium
- Has surpassed MRSA as most common nosocomial (hospital-acquired) disease

Scientific Classification
Kingdom |
Bacteria |
Phylum |
Firmicutes |
Class |
Clostridia |
Order |
Clostridiales |
Family |
Clostridiaceae |
Genus |
Clostridium |
Species |
C. difficile |
Where it lives
- Intestinal tract of healthy people
- 13.6% of children, 5.5% of adults are colonized
Tetro, J. Clostridium difficile Is More Common Than You Think (2016)
- 70% of infants < 10-12 months old carry C. diff
Lamont, T. C. diff in 30 Minutes. (2017)
- 13.6% of children, 5.5% of adults are colonized
- Soil
- Water
- Feces of infected animals and humans
- Surfaces for up to 5 months
Signs / Symptoms
- Diarrhea
- Fever
- Nausea
- Abdominal pain
- Pseudomembranous colitis
- Toxic megacolon
- Perforation of the colon
- Sepsis
CDI risk
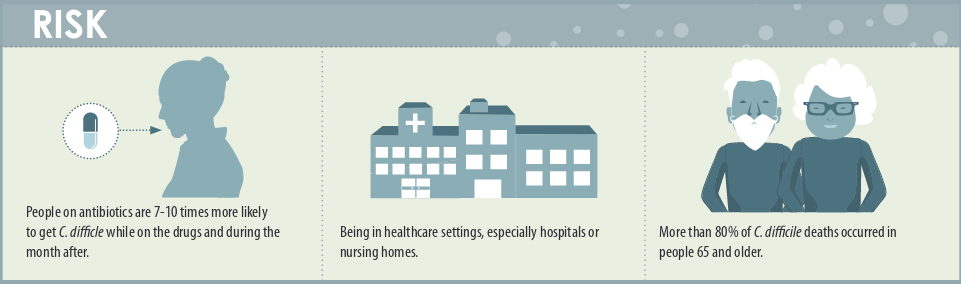
How CDI spreads

CDI treatments
- Antibiotics
- Flagyl (metronidazole) - Cheap, no longer recommended
- Vanco (vancomycin) - Expensive but effective
- Dificid (fidaxomicin) - Most expensive, most effective
Louie, T., et. al. Fidaxomicin versus Vancomycin for Clostridium difficile Infection. (2011)
- Fecal Microbiota Transplants (FMT)
- via ng-tube or colonoscopy (similar outcomes)
Postigo, R. and Kim, J.H. Colonoscopic versus nasogastric fecal transplantation for the treatment of Clostridium difficile infection: a review and pooled analysis. (2012)
- via OpenBiome capsules
- via ng-tube or colonoscopy (similar outcomes)
- Probiotics are not recommended
Renal (kidney) disease
- Acute kidney injury (AKI)
- Chronic kidney disease
- Stages 1-4
- Stage 5 - End-stage renal disease (ESRD)
- Dialysis or transplant
Renal disease signs / symptoms
- Nausea
- Vomiting
- Loss of appetite
- Fatigue and weakness
- Sleep problems
- Changes in urine volume
- …much more
Renal disease treatments
- Treat the underlying cause
AKI Causes
- Decreased blood flow
- Direct damage to kidneys
- Urinary tract blockage
AKI Risks
- Hospitalization
- Advanced age
- Blood vessel blockage in arms/legs
- Diabetes
- High blood pressure
- Heart failure
- Kidney diseases
- Liver diseases
CKD Causes
- Type I/II diabetes
- High blood pressure
- …much more
CKD risk
- Cardiovascular disease
- Smoking
- Obesity
- Race
- African-, Native-, or Asian-American
- Family history of kidney disease
- Abnormal kidney structure
- Older age
Measuring kidney function
- Glomerular Filtration Rate (GFR)
- MDRD
\[ GFR = 175 \times S_{cr} - 1.154 \times \text{Age}^{-0.203} \times 0.742 \cdot I(\text{F}) \times 1.212 \cdot I(\text{AA}) \]
- CKD-EPI
\[ GFR = 141 \times min\bigg(\frac{S_{cr}}{\kappa}, 1\bigg)^{\alpha} \times max\bigg(\frac{S_{cr}}{\kappa}, 1\bigg)^{-1.209} \\ \times 0.993^{\text{Age}} \times 1.018 \cdot \text{I}(\text{F}) \times 1.159 \cdot \text{I}(\text{AA}) \]
- F is female sex
- AA is African American race
- I is 1 if true, else reciprocal of preceding term
- \(S_{cr}\) is serum creatinine in mg/dL
- \(\kappa\) is 0.7 for females and 0.9 for males
- \(\alpha\) is -0.329 for females and -0.411 for males
CKD Stages
| Stage | Description | GFR/Kidney Function |
|---|---|---|
1 |
Normal function |
90+/90%+ |
2 |
Mild loss |
60-89/60-89% |
3 |
Mild to severe |
30-59/30-59% |
4 |
Severe |
15-29/15-29% |
5 |
Kidney failure (ESRD) |
15 or less/15% or less |
End-stage renal disease (ESRD)
- When stage 5 is reached
- Dialysis or kidney transplant
Readmissions
- If hospital has “excess readmissions”, penalties are assessed
- 30-day risk standardized measure to calculate Payment Readjustment Factor (PRF)
All-cause unplanned readmissions to the same or another applicable acute care hospital, occurring within 30 days - for any reason, regardless of principal diagnosis - from the index admission are counted in this measure. Some planned readmissions are not counted. HRRP
\[ \text{PRF} = 1 - min\bigg(0.03, \sum_{dx} \frac{\text{Payment}(dx) \cdot max\big((\text{ERR}(dx) - 1.0), 0\big)}{\text{All payments}}\bigg) \]
- Where \(dx\) is one of six measure cohorts, incl heart failure, pneumonia, et. al.
- ERR is a hospital’s performance measure \(dx\), and payment refers to base operating DRG payments.
The data
A fun experiment
- Step 1: Pick a random percentage. e.g. 54%, 28%, 77%, etc.
- Step 2: Type that number into Google followed by “of Americans”
- Step 3: Follow rabbit hole for hours
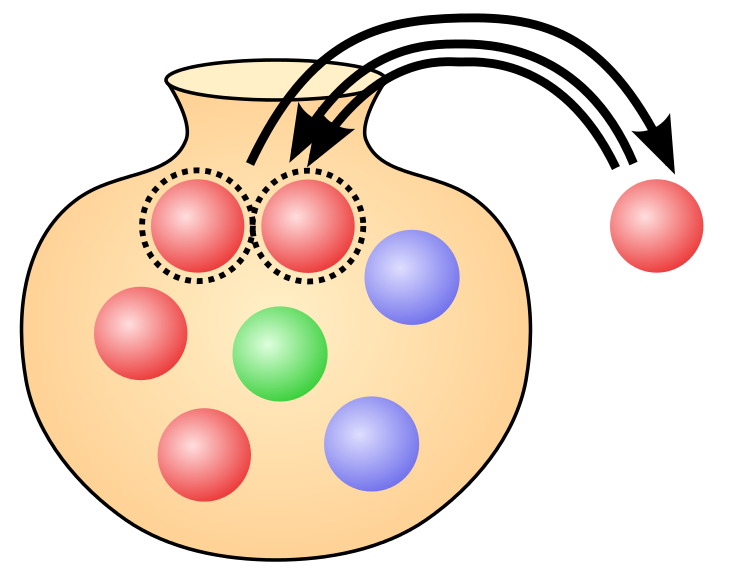
Simple random sample
- Pólya urn model
- With (SRSWR) or Without Replacement (SRSWOR)
- With replacement - makes use of i.i.d. assumption
- Without replacement - not i.i.d. but still exchangeable
- Requires access to the entire population
Sampling design
| Sampling Plan | Design-based inference | Model-based inference |
|---|---|---|
Probability sample |
A |
C |
Model-dependent sample |
B |
D |
Quota sampling |
E |
F |
Convenience sampling |
G |
H |
Snowball sampling |
I |
J |
Peer nomination |
K |
L |
Design effects
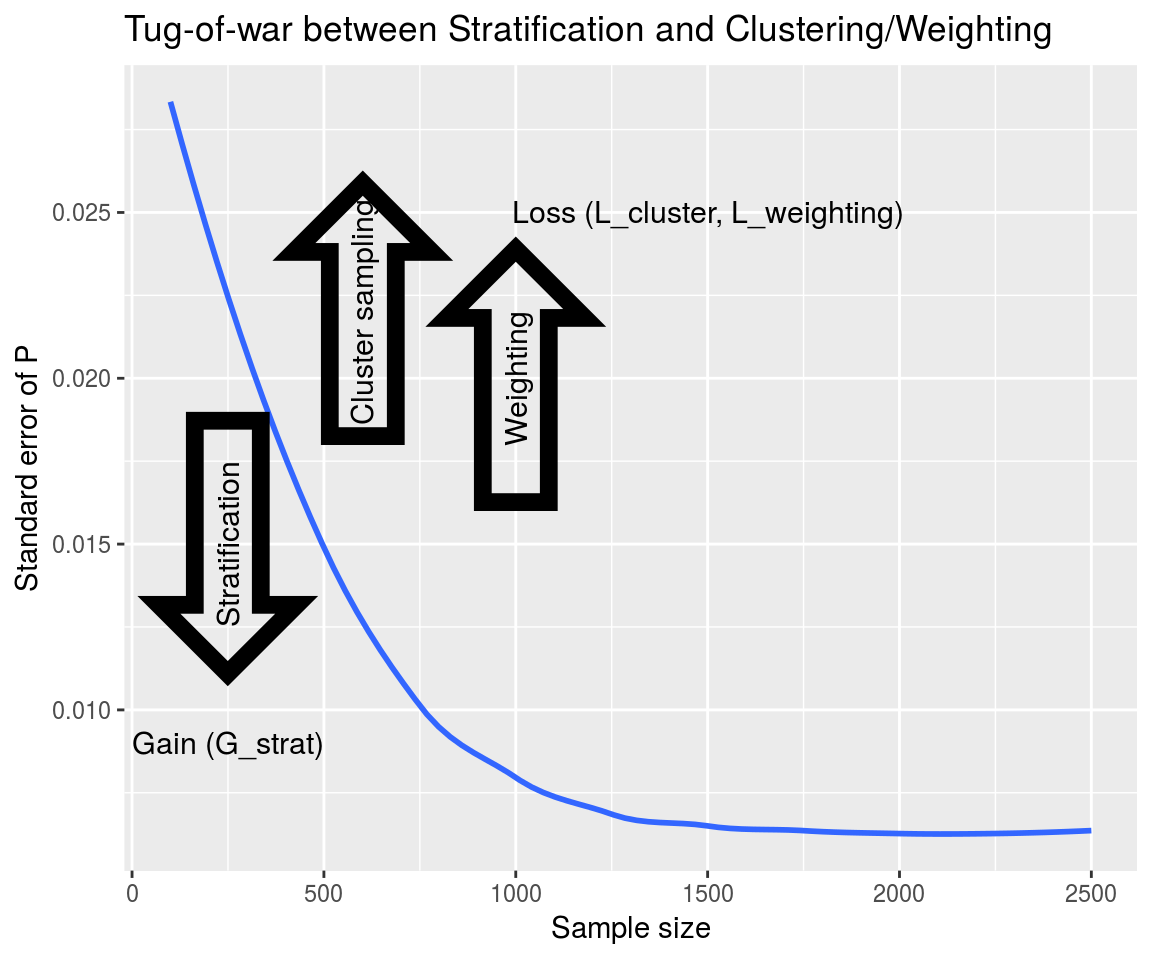
Design effects
- “deft”
- Similar to variance inflation factor (VIF)
- Effective sample size
\[ D^2(\hat{\theta}) = \frac{SE(\hat{\theta})^2_{complex}}{SE(\hat{\theta})^2_{srs}} = \frac{var(\hat{\theta})_{complex}}{var(\hat{\theta})_{srs}} \]
\[ n_{eff} = \frac{n_{complex}}{d^2(\hat{\theta})} \]
Clustering
- Grouping people by geographic regions
- SRS to choose a geographic region

Clustering

Stratification

Stratification

Weighting
- \(N = 51\)

Weighting
- \(N_{men} = 30\)
- \(p_{men} = \frac{30}{51} = 0.588\)

Weighting
- \(N_{women} = 21\)
- \(p_{women} = \frac{21}{51} = 0.412\)
Weighting
- \(N_{women} = 21\)
- Women Odds Ratio: \(\frac{p_{women}}{p_{men}} = \frac{0.588}{0.412} = 1.427\)
- Men Odds Ratio: \(\frac{p_{men}}{p_{women}} = \frac{0.412}{0.588} = 0.701\)
H-CUP Databases
- Healthcare Cost and Utilization Project
- Includes NIS and NRD
- Must be purchased
- Data usage agreement required for analysts
NIS Sampling Design
- Nationwide Inpatient Sample
- 1988-2011: 100% sample of 20% of HCUP hospitals
- National Inpatient Sample
- 2012-present: 20% sample of 100% of HCUP hospitals
HCUP Complex Survey Design
- Clustered on hospital ID
- Weights included in
discwtfield for national estimates - 1988-2011: Stratified by census region and bed size
- 2012-present: Stratified by census division and bedside
- Region 1 (Northeast)
- Division 1 (New England) -Division 2 (Mid Atlantic)
- Region 2 (Midwest)
- Division 3 (East North Central)
- Division 4 (West North Central) (incl. Nebraska)
- Region 3 (South)
- Division 5 (South Atlantic)
- Division 6 (East South Central)
- Division 7 (West South Central)
- Region 4 (West)
- Division 8 (Mountain)
- Division 9 (Pacific)
- Region 1 (Northeast)
Importance of survey design
- Treating as SRS
summary(lm(los~age, data=cdiff))##
## Call:
## lm(formula = los ~ age, data = cdiff)
##
## Residuals:
## Min 1Q Median 3Q Max
## -14.19 -7.12 -3.98 2.27 349.01
##
## Coefficients:
## Estimate Std. Error t value Pr(>|t|)
## (Intercept) 14.190744 0.187955 75.50 <0.0000000000000002 ***
## age -0.043275 0.002687 -16.11 <0.0000000000000002 ***
## ---
## Signif. codes: 0 '***' 0.001 '**' 0.01 '*' 0.05 '.' 0.1 ' ' 1
##
## Residual standard error: 13.94 on 73264 degrees of freedom
## Multiple R-squared: 0.003528, Adjusted R-squared: 0.003514
## F-statistic: 259.4 on 1 and 73264 DF, p-value: < 0.00000000000000022Importance of survey design
- Accounting for survey design with R survey package
library('survey')
cdiff.design <- svydesign(ids = ~hospid, data = cdiff, weights = ~discwt, strata = ~nis_stratum, nest=TRUE)
summary(svyglm(los~age, design=cdiff.design))##
## Call:
## svyglm(formula = los ~ age, design = cdiff.design)
##
## Survey design:
## svydesign(ids = ~hospid, data = cdiff, weights = ~discwt, strata = ~nis_stratum,
## nest = TRUE)
##
## Coefficients:
## Estimate Std. Error t value Pr(>|t|)
## (Intercept) 13.95231 0.55033 25.353 < 0.0000000000000002 ***
## age -0.04657 0.00637 -7.311 0.000000000000627 ***
## ---
## Signif. codes: 0 '***' 0.001 '**' 0.01 '*' 0.05 '.' 0.1 ' ' 1
##
## (Dispersion parameter for gaussian family taken to be 180.579)
##
## Number of Fisher Scoring iterations: 2SRS vs. complex design
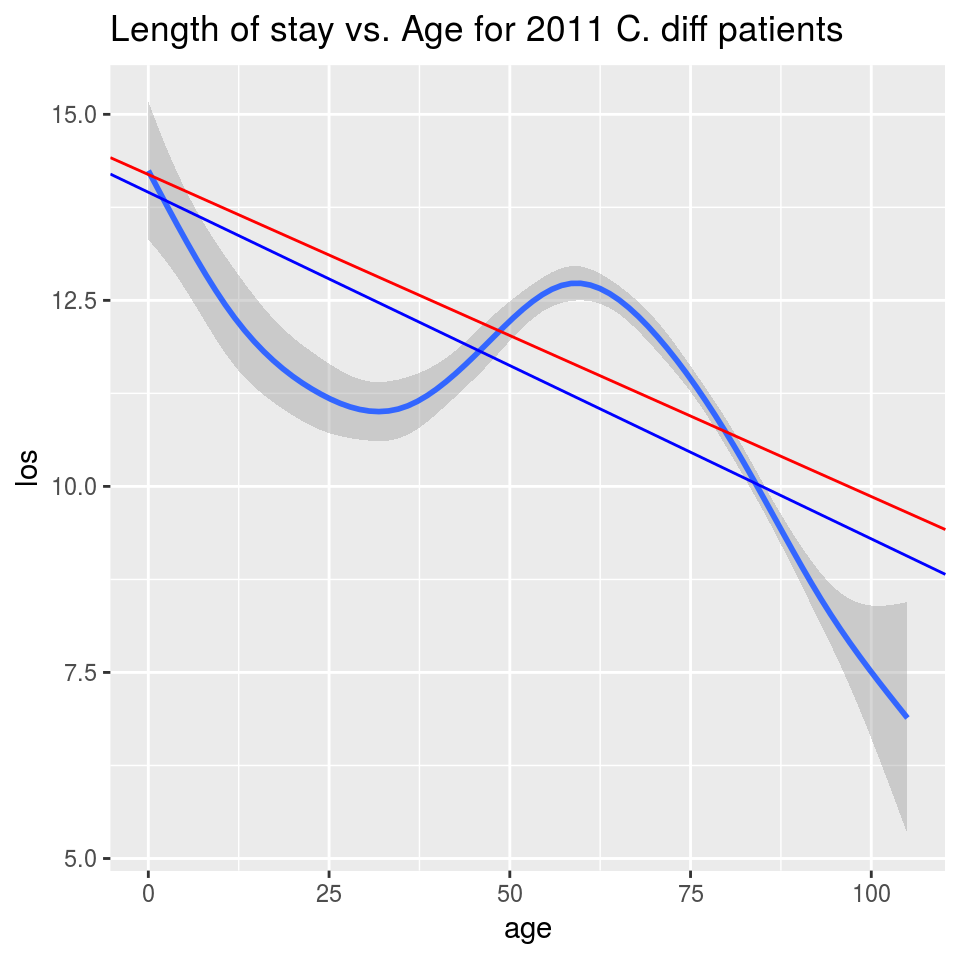
SRS line in red, complex design in blue
Research design checklist
- Only detect disease conditions, procedures, and diagnostic tests in hospital settings
- “Encounters” not patients
- No volume-specific assessments for:
- Geographic units, like U.S. states
- Healthcare facilities (after 2011)
- Individual health care providers
- Determine diseases and procedures using validated administrative codes
- Limit assessment to in-hospital outcomes
- Distinguish between complications and comorbidities or state where you cannot
- Account for NIS/NRD survey design
- Address changes in data structure over time for trend analysis
NIS Features
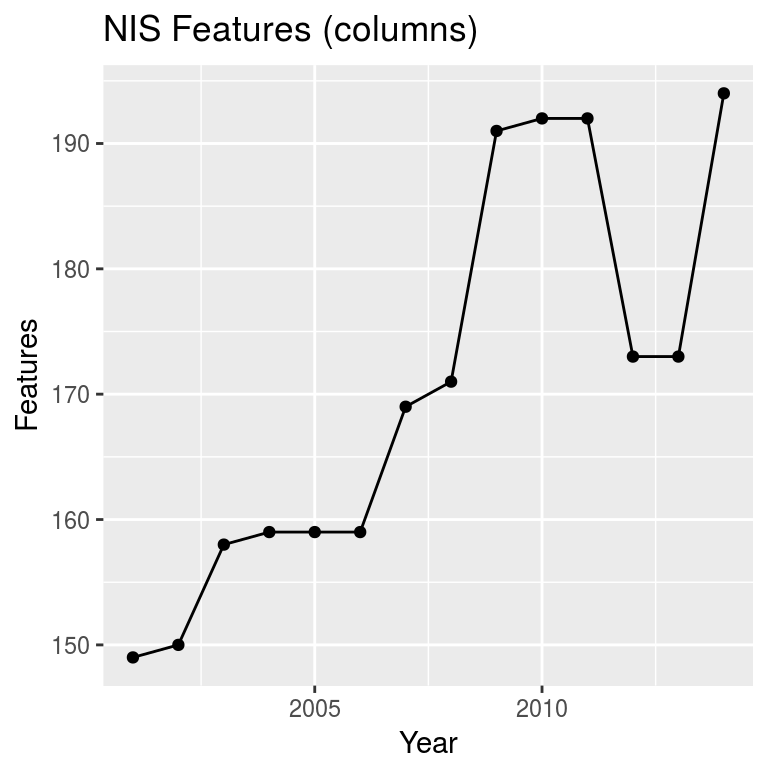
- 2009 - Added DX and DXCCS codes 16-25
- 2012 - NIS redesign (removed hospital-specific features)
- 2014 - Added DX and DXCCS codes 26-30
NIS dimensions
- Big data?
- Definitely large data
- ~3 GB per year (raw CSV)
- 108,683,763 total rows
- 10868376.3 per year
NRD Features
- Years 2010-2013 had 116 features
- 2014 had 126 features
- Added DX and DXCCS 26-30
- ~10 GB per year (raw CSV)
- 87,699,909
- 17539981.8 per year
Features of interest
- Age
- Female
- Length of Stay
- Died
- Hospital categorization
- DXn codes (ICD-9-CM codes)
- C. diff - 00845
- AKI - 584, 584.5-584.9
- CKD - 585, 585.1-585.6, 585.9
- Renal Failure, unspecified - 586
Methodology
Dealing with big data
![]()
- Column-store relational database
- Data warehouse
Getting data into the database
- Lots of Excel work
- NIS CSV: ~3GB
- read_csv(…NIS…): ~64 GB in RAM
- NRD CSV: ~6GB
- read_csv(…NRD…): CRASHED
- Had to split data
Getting data back out
SELECT *
FROM nis
WHERE nis.dx1 = '00845'
OR nis.dx2 = '00845'
OR nis.dx3 = '00845'
OR nis.dx4 = '00845'
OR nis.dx5 = '00845'
OR nis.dx6 = '00845'
OR nis.dx7 = '00845'
OR nis.dx8 = '00845'
OR nis.dx9 = '00845'
OR nis.dx10 = '00845'
OR nis.dx11 = '00845'
OR nis.dx12 = '00845'
OR nis.dx13 = '00845'
OR nis.dx14 = '00845'
OR nis.dx15 = '00845'
OR nis.dx16 = '00845'
OR nis.dx17 = '00845'
OR nis.dx18 = '00845'
OR nis.dx19 = '00845'
OR nis.dx20 = '00845'
OR nis.dx21 = '00845'
OR nis.dx22 = '00845'
OR nis.dx23 = '00845'
OR nis.dx23 = '00845'
OR nis.dx25 = '00845'
OR nis.dx26 = '00845'
OR nis.dx27 = '00845'
OR nis.dx28 = '00845'
OR nis.dx29 = '00845'
OR nis.dx30 = '00845'Readmissions
- nrd_visitlink allows analyst to link visits
- los and nrd_daystoevent used to determine sequence and length of stay
- Up to analyst to determine “index” admission and readmissions
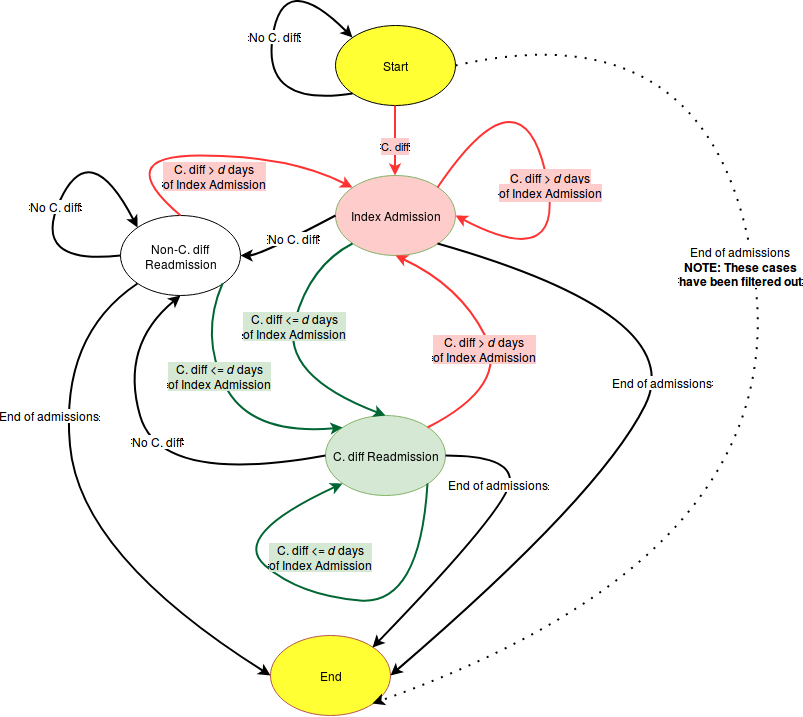
Other considerations
- 2010-2014: (1 ≤ DMONTH ≤ 12 − ceil(d/30))
- Cut off index events with enough time to track readmissions
- DIED \(\ne\) 0
- A death on index does not allow for readmission
- Length of stay > 0
- LOS == zero represents transfers and same-day stays (more complex)
- AGE > 0
- Infants are often asymptomatic carriers of C. diff
Models
- Linear logistic regression
- Start with all C. diff patients
- Fit each year separately
- Accounts for changes in years
- Allowed fitting to complete under hardware limitations
readmitted ~ hosp_hcontrl_govt +
hosp_hcontrl_priv_np +
hosp_urcat4 +
hosp_ur_teach_metro +
hosp_ur_teach_metro_teaching +
hosp_bedsize +
female +
acute_kidney_failure +
chronic_kidney_disease2 +
chronic_kidney_disease3 +
chronic_kidney_disease4 +
chronic_kidney_disease5 +
chronic_kidney_disease6 +
chronic_kidney_disease_unk +
renal_failure_unspecifiedResults
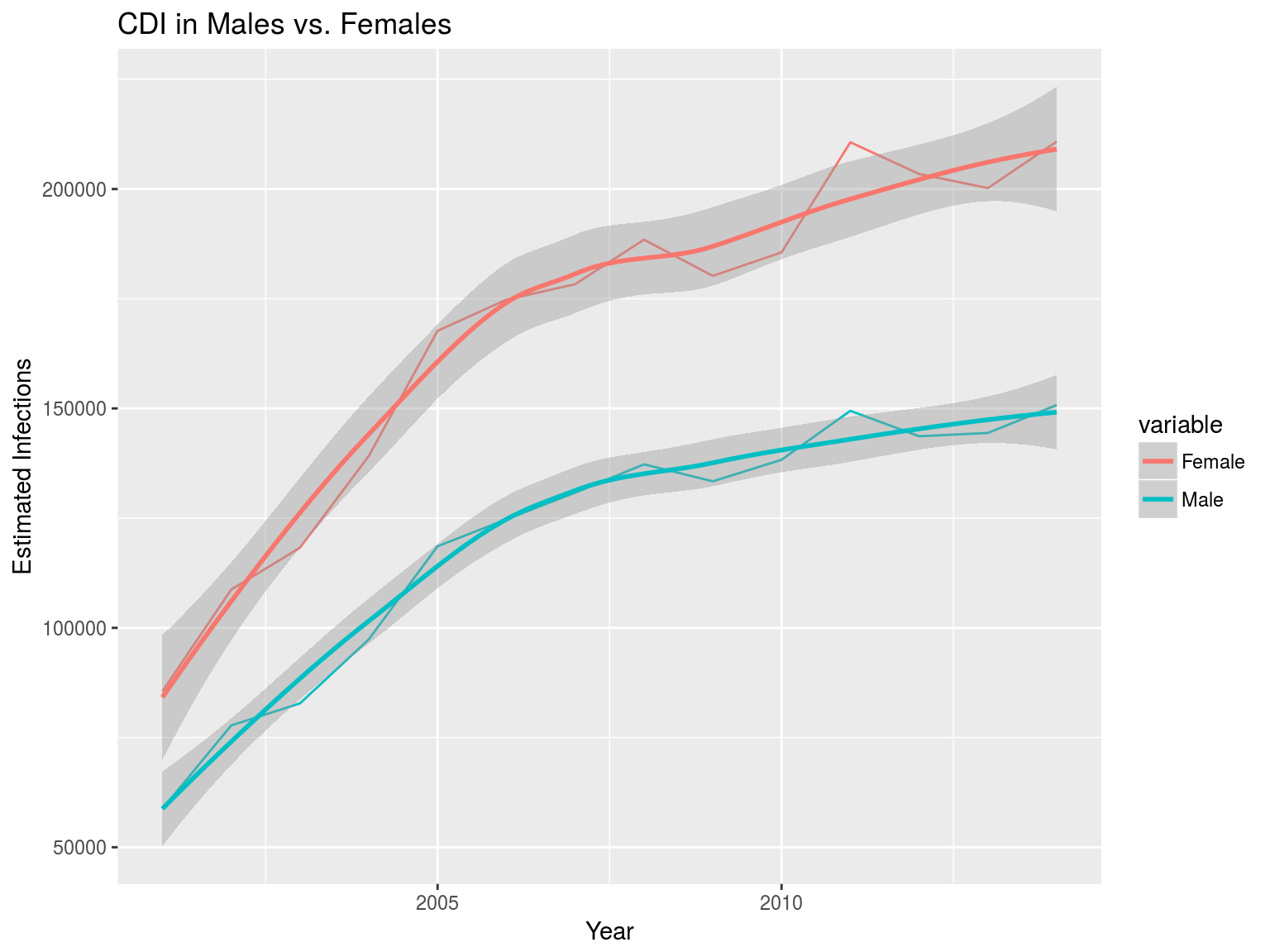
Trends
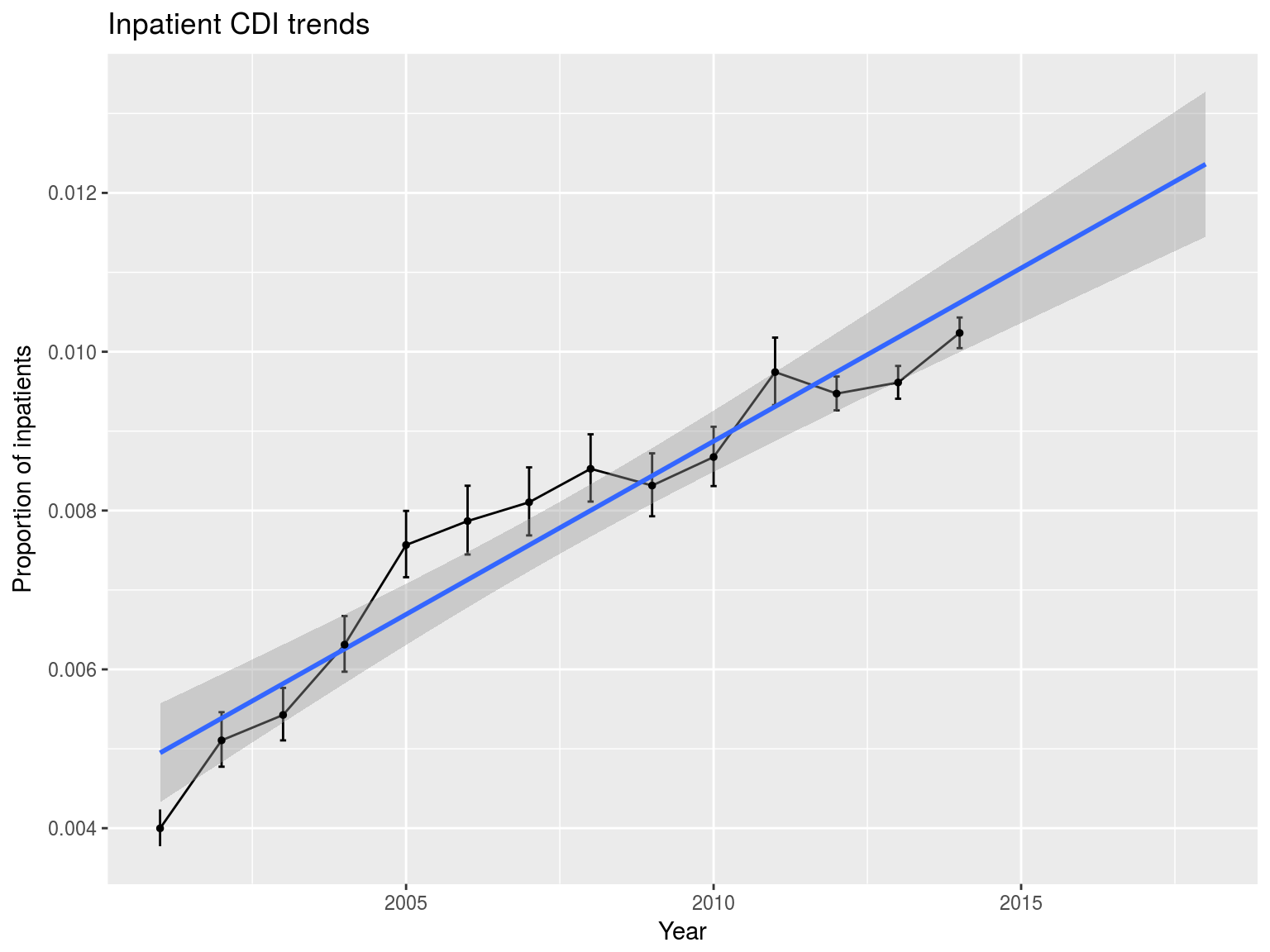
Trends
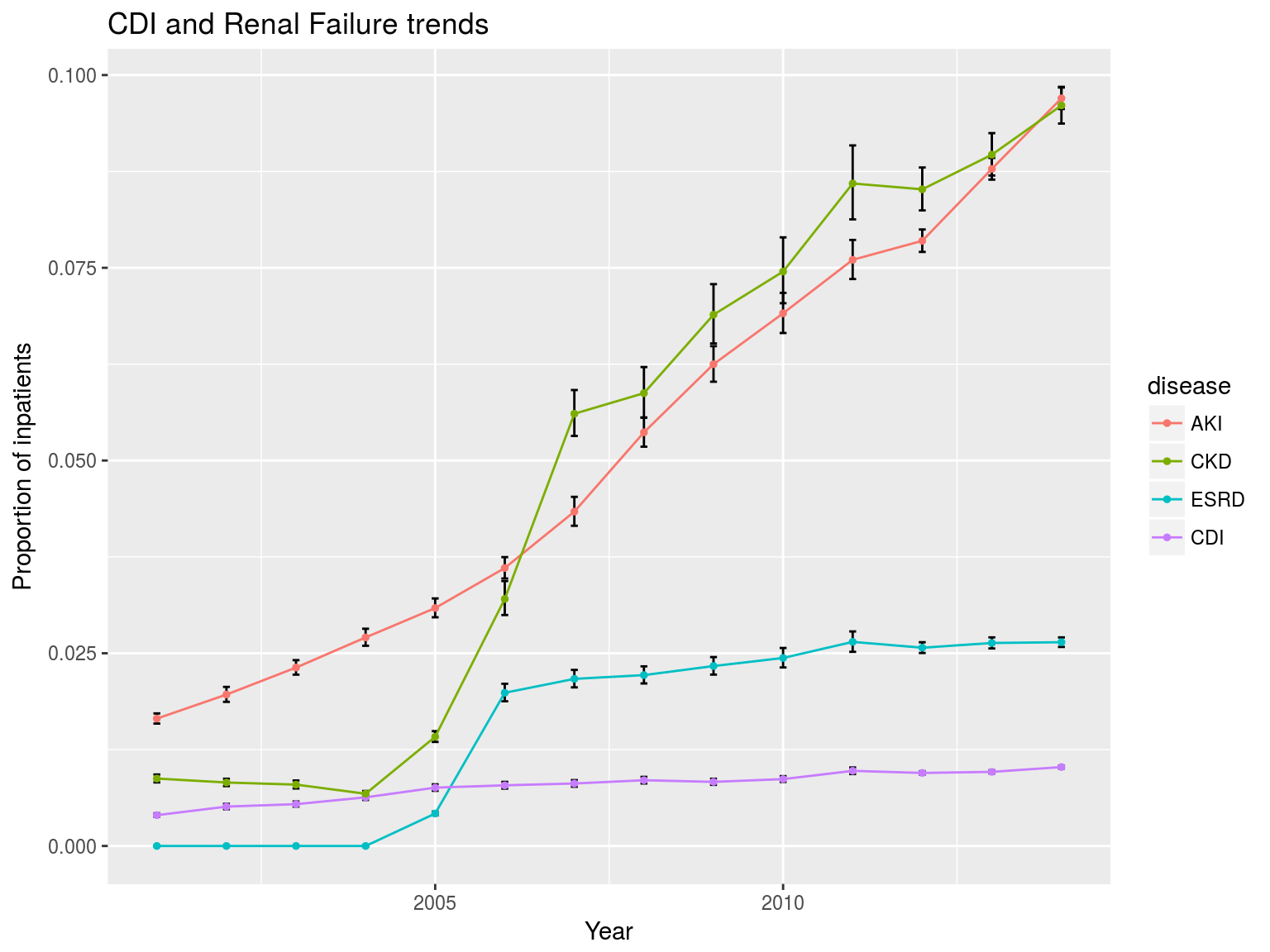
Trends
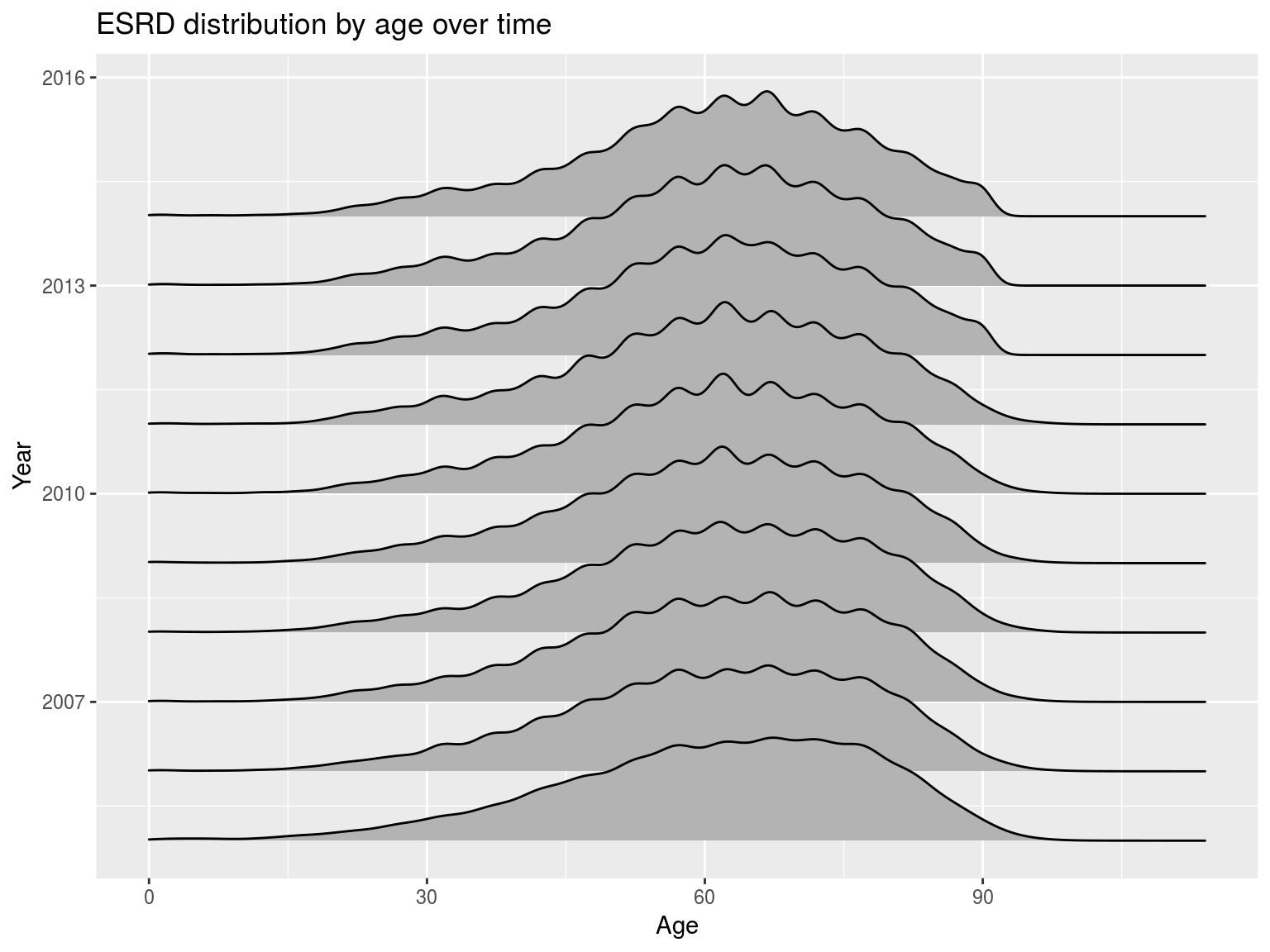
Trends
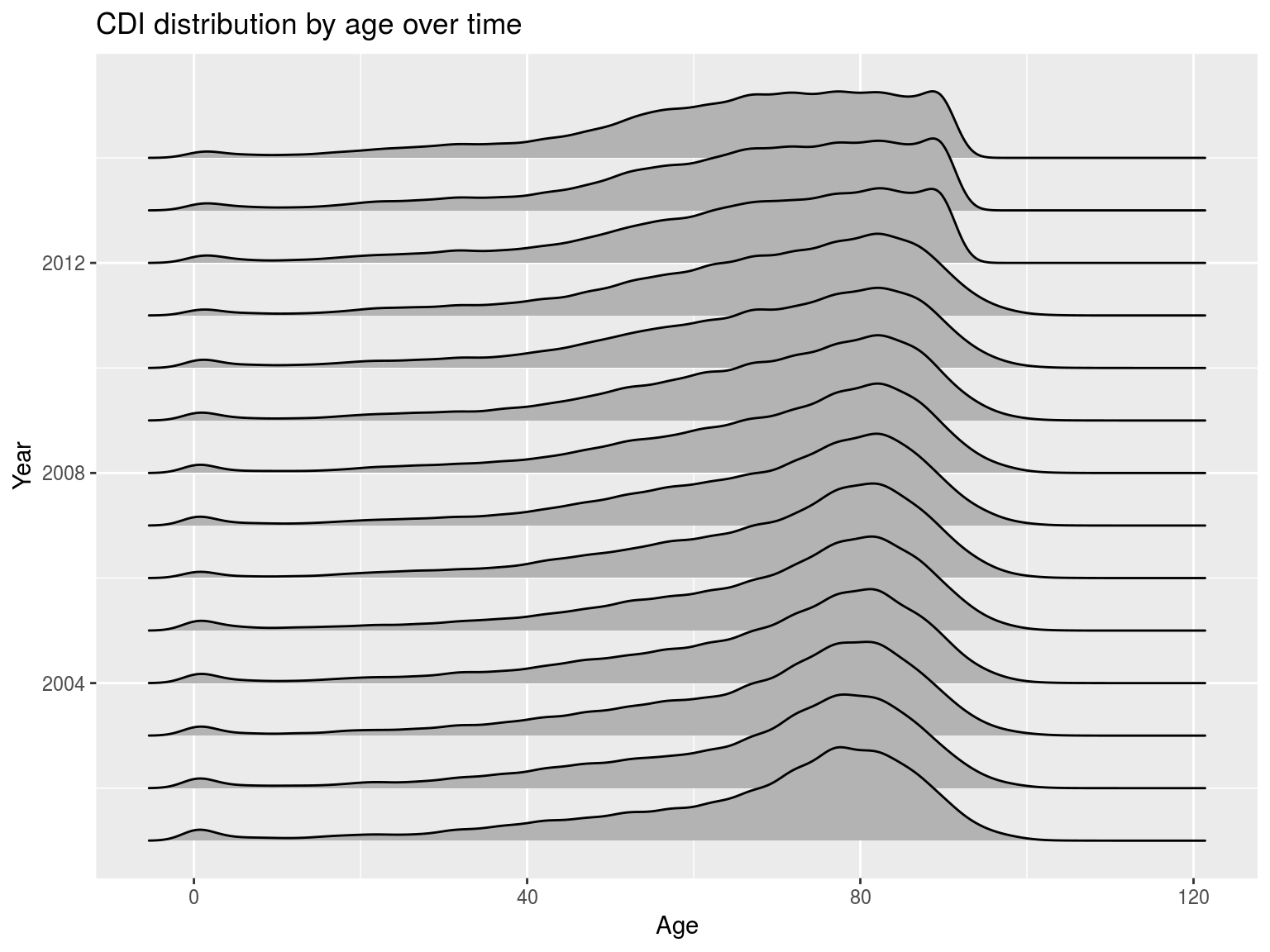
Trends
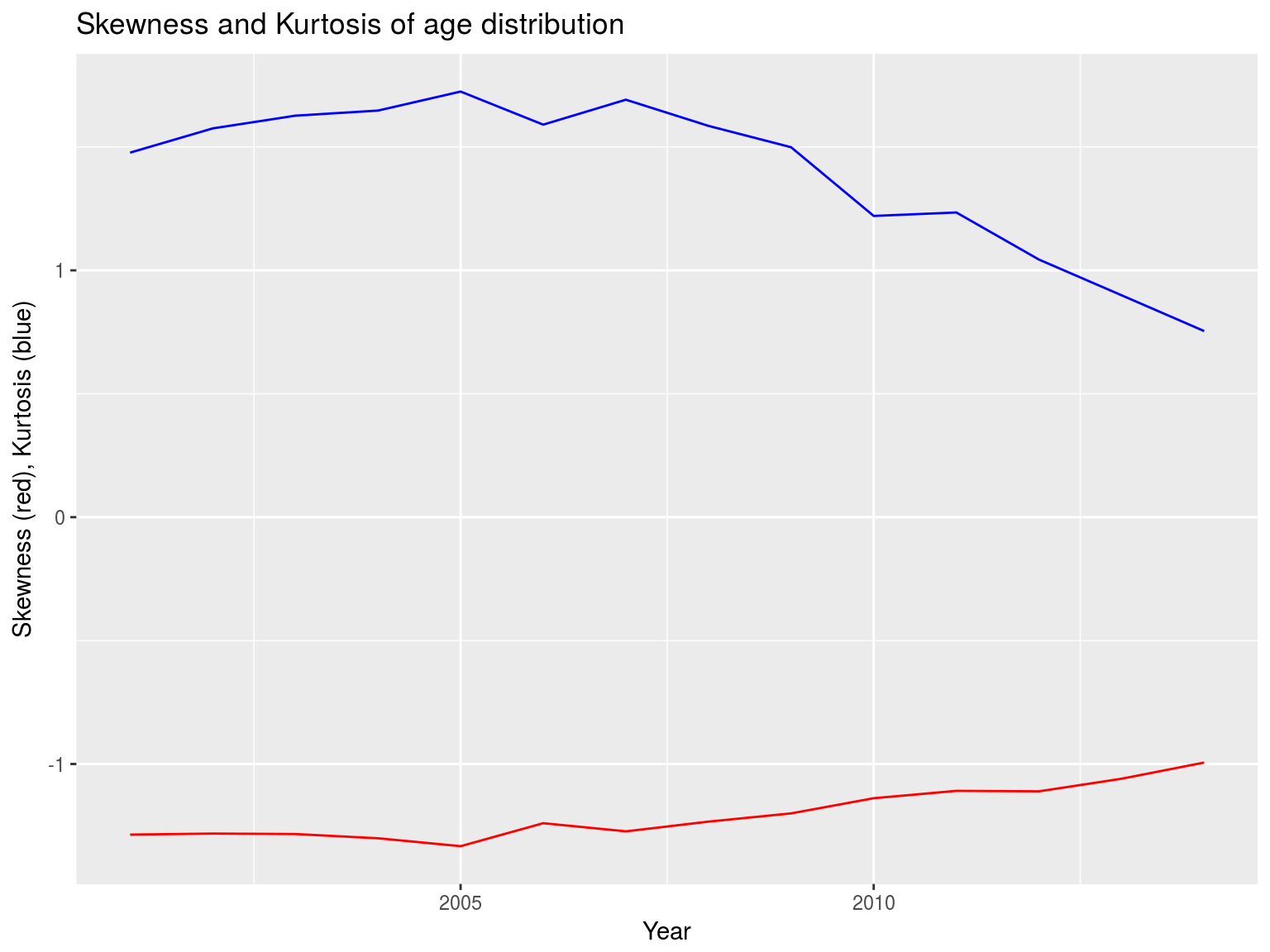
Trends
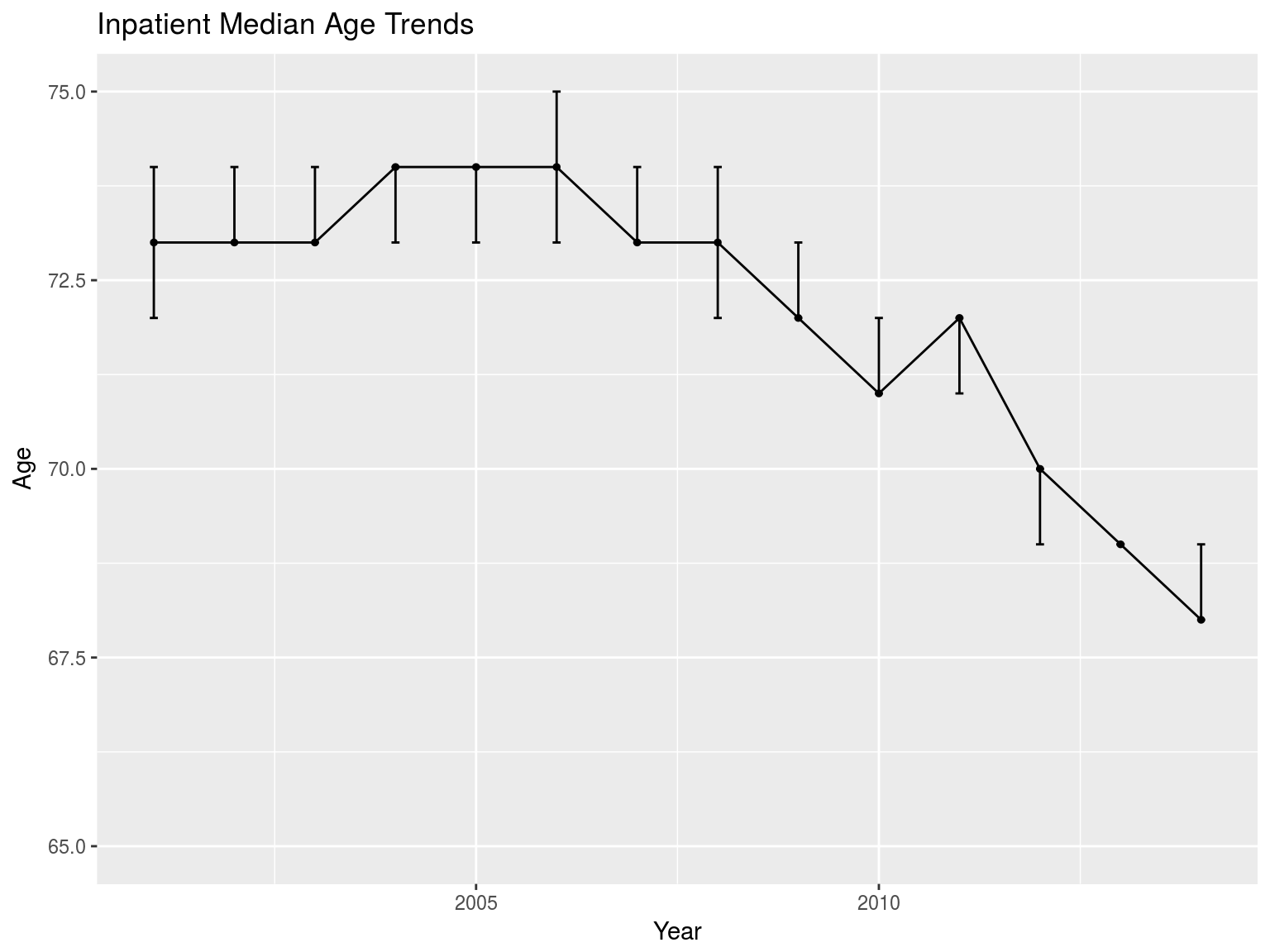
Trends
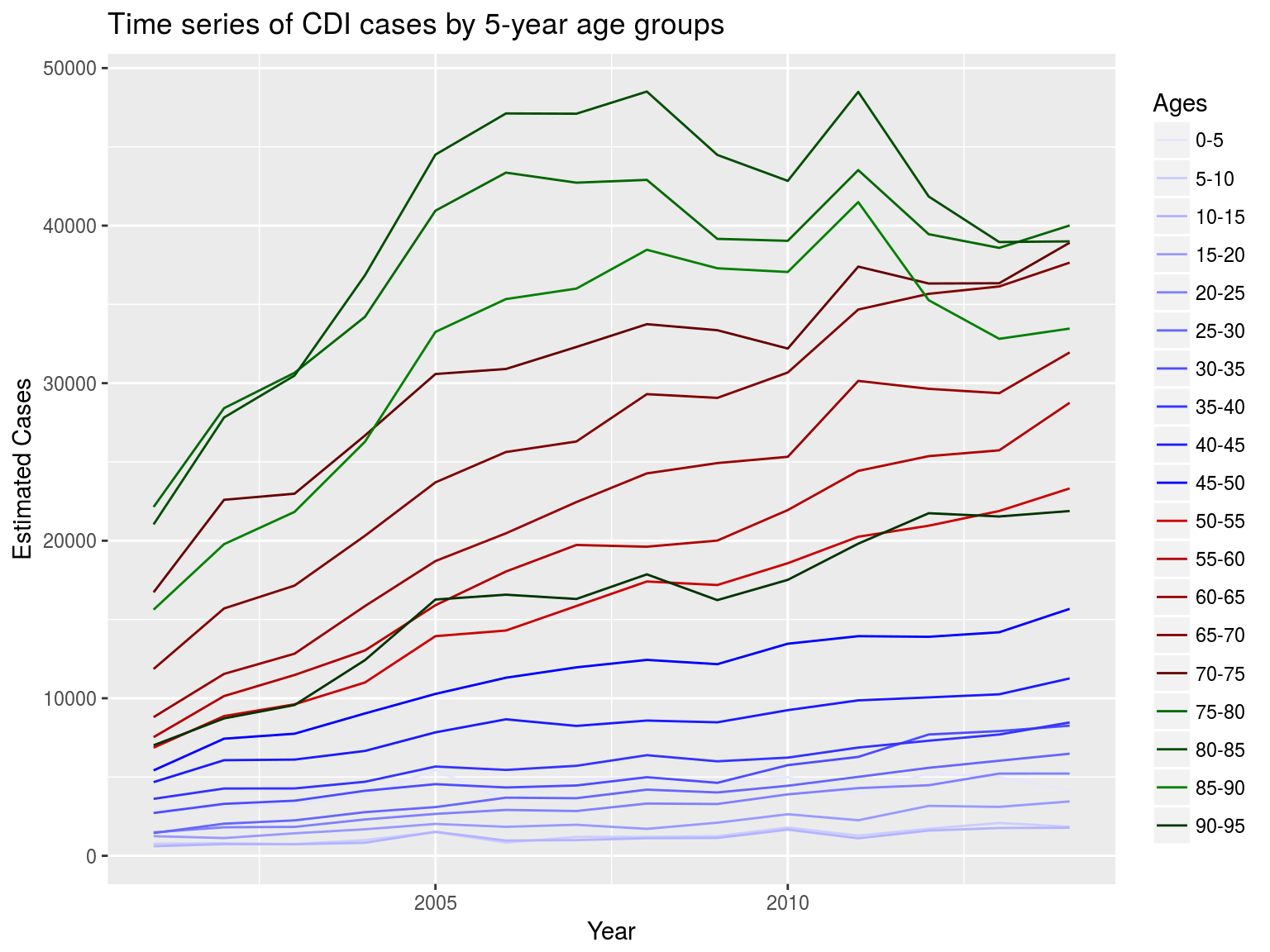
Trends
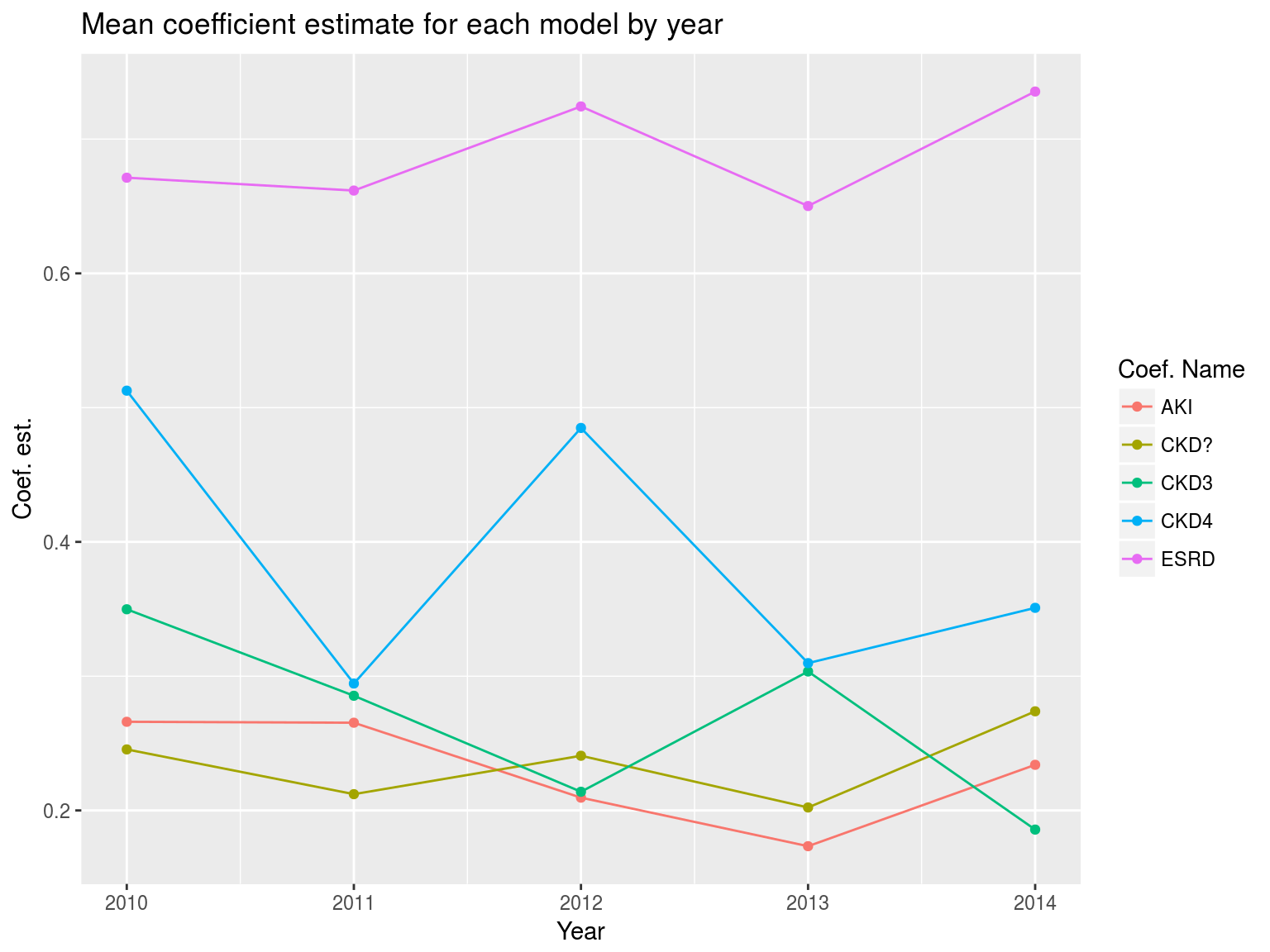
Model fit
Conclusions
- CDI spreading into younger demographics
- Age - correlation or causation?
- Other comorbidities associated with age
- ESRD, AKI, and some CKD stages strong predictors for CDI readmission
Future work
- Age as a risk factor?
- What is causing spread into younger groups?
- Why are females more likely to get CDI?
- Mortality?
- Treatment studies?
Acknowledgements
Very special thanks
- Renuga Vivekanandan, M.D.
- Ryan Walters, Ph.D.
- Dora Matache, Ph.D.
Thank you!
